Physical pain is common. Everyone will experience it at some point in his or her life. Often, pain will result from an injury and will resolve when the injury heals. This is normal. This is good news for the 84% of us who will likely experience something like low back pain in our lives. It will come and go and we will go on our marry way. But for many, this pain lingers and has become the most common cause of disability and time off work in people over the age of 45 (Balagué et al. 2012). Long term, or chronic pain, that results in disability is a much bigger issue. What’s worse is that many of these people end up relying on opioid drugs (prescription and not) in attempts to manage their pain.
Opioids and the crisis
Opioid use has sky-rocketed in recent years, and drug overdose deaths are on the rise. So much so that the Center for Disease Control (CDC) has declared that we are in the middle of an “opioid crisis” and it is an epidemic. This epidemic is not just affecting the heroin addict living in the back alley. It’s everyday people who rely on opioids to cope with pain (i.e., low back pain, knee pain). The statistics are staggering:
- From 1999 to 2017, more than 700,000 people have died from drug overdose.
- Around 68% of the more than 70,200 drug overdose deaths in 2017 involved an opioid.
- In 2017, the number of overdose deaths involving opioids (including prescription opioids and illegal opioids like heroin and illicitly manufactured fentanyl) was 6 times higher than in 1999.
State by State Look at Opioid Statistics
Despite this, it is important to note that THERE IS a time and place for taking opioids—for instance, following significant surgery or injury when managing pain is difficult without them. However, prolonged use of opioids long after recovery from surgery or traumatic injury can result in addiction and can cause people to rely on opioids long term. The reason that people become addicted to opioids is that they only mask the sensation of pain—they do not alter the source of the pain. This is not to mention that the withdrawal symptoms are severe. It’s hard to get off of opioids. This is the vicious cycle of addiction. Taking opioids long term also has side effects of depression, for which many people take more drugs. This is why there are important Questions to ask your doctor about pain medication when they are writing you a prescription. Even the most well-meaning doctors can send you down the road of addiction without meaning to.
Long story short, opioids are a “bandaid” for pain and getting to the root of the problem requires understanding why someone enters a state of chronic pain. If an injury is healed and there is no more tissue damage or new injury, then why can one still hurt? This is what is important to get a handle on. Many factors play a role in creating each person’s unique “pain experience” which includes emotions, thoughts and beliefs—it’s not just physical. Read on…
Understanding Pain
Research has shown that when people understand pain, they can better manage their pain. And when one can manage his or her own pain, he or she can take life by the horns again. Simply put:
“Know pain, know gain”—David Butler
This is especially true for people dealing with chronic pain. Many people have an overly simplistic view of how pain is experienced. And I say “experienced” very deliberately. As children, we learn that doing something such as touching a hot stove or stepping on a sharp object with bare feet creates pain. These two events are generally associated with tissue damage—the skin is compromised and you get a blister or a stab wound. But the shocking thing to most people is that this pain does not originate in the injured part of the body. Pain is an experience that is created in the brain once it interprets the signals that the rest of the body send to it. So when you step on a nail, the sensory cells send signals all the way up the spinal cord to your brain where you brain interprets this event as being painful. Obviously, this occurs in fractions of second and you generally pull your foot away from the nail. In this experience, the interpretation of pain is a good thing—it signifies that there is a threat in your environment (the nail) that you harm you.
The fact that pain is an experience that is created by the brain explains why two soccer players can experience the same injury on the field and one gets up and keeps playing while the other lays on the ground crying out for help. It also explains why people can experience pain in a body part without actual threat to it. Say you had a traumatic experience as a child when you stepped on a rusty nail with bare feet and you ended up in the hospital with pain and a raging infection in your foot. Now, when you so much as look at a rusty nail you experience pain in your foot. You foot is healed and the nail is no where near your foot. Danger is absent, injury is absent……but pain is ever present. This experience is created purely in the brain.
Below are a few videos from some of the World’s leading pain experts. Watch them to learn more about how your pain experience is created ….. and how you can take control.
Below, Professor Lorimer Mosely explains how pain works. Pain evolved as a protective mechanism to indicate when the body was in danger. However, when our experiences change the way that pain is experienced and skews what the pain is indicating, it can result in a maladaptive response—or extreme fear from harmless sensation (i.e., a tree branch brushing one’s leg on a hike).
Each part of your body is represented on a specific area of the brain. There is a part of your brain dedicated to being able to detect sensation of your left pinky finger—and every other part of your body. If you experience prolonged pain in your left pinky finger, the “sharpness” of left pinky’s representation on the brain is lost and you brain can no longer create a pain experience in just your left pinky. Maybe then your neighboring fingers begin to hurt and the pain becomes more widespread. This is phenomena is known as brian smudging as explained below by expert David Butler.
If you have recurring or ruminating thoughts of your pain, that is a sure recipe for making your pain worse. Yes—pain has a significant emotional component. These recurring thoughts have been termed “thought viruses”.
Myth: getting high tech imaging of your painful area will explain the source of your pain.
Professor Peter O’Sullivan explains the discrepancy between medical imaging and pain and how thoughts, and beliefs and movement habits actually matter more.
It’s only 1% of back pain that is really serious stuff….99% has no diagnosis based on scan”. Peter O’Sullivan.
Physical Therapy is a safe alternative to opioids for pain management
If you watched the video above with Professor Peter O’Sullivan, you will have learned that many people with low back pain get medical imaging (i.e., MRI, X-rays, CT scans) that lead them to believe that their backs were really “messed up” structurally. As a result, they developed fear of further injury and starting moving (or not moving) in ways that actually exacerbated their pain—-it wasn’t the “bulging disc” that might have been found on imaging.
“Pain does not equal structural injury” –Prof. Peter O’Sullivan
Restoring healthy movement patterns in conjunction with understanding pain is essential to managing back pain. Physical therapists can help you do both. Even better, physical therapy can not only get you moving better again, they can get you back to an more active lifestyle that includes activities that you love doing. This is why the CDC has recommended physical therapy as a safe alternative to opioids for pain management.



Resources for helping managing chronic pain have been compiled by the ChoosePT movement organized by the American Physical Therapy Association (APTA).
7 tips from the ChoosePT movement for managing chronic pain
If you would like to delve deeper into these topics, here are two books that I would highly recommend. Click on the images to see details.


Weber Physical Therapy and Wellness supports the ChoosePT movement. If you are experiencing chronic pain and would like a free consult to see how physical therapy can help you, please get in touch or schedule a free consultation:
Schedule Appointment
***
References and helpful websites:
Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. The Lancet. 2012;4(379): 482-91.
Rundell SD, Davenport TE. Patient education based on principles of cognitive behavioral therapy for a patient with persistent low back pain: a case report. J Orthop Sports Phys Ther. 2010:40:494–501.
Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis [erratum in: N Engl J Med. 2013;369:683]. N Engl J Med. 2013;368:1675-1684.
Longo UG, Franceschi F, Berton A, et al. Conservative treatment and rotator cuff tear progression. Med Sport Sci. 2012;57:90–99.
http://www.pain-ed.com/blog/2019/09/09/can-the-way-we-move-after-injury-lead-to-chronic-pain/
https://www.noigroup.com/about/
https://www.cdc.gov/drugoverdose/epidemic/index.html
https://www.choosept.com/choose-physical-therapy-over-opioids-for-pain-management-choosept
 Running is stressful on the body and so is child-birth. Doing these two things too closely back to back can have adverse consequences. This is evidenced by the prevalence of urinary incontinence, pelvic organ prolapse (POP), abdominal muscle separation and pain that are experienced by female runners after having a baby. Urinary incontinence and POP can result from the stress that is place on the pelvic floor muscles. For a review of the anatomy of the pelvic floor muscles click
Running is stressful on the body and so is child-birth. Doing these two things too closely back to back can have adverse consequences. This is evidenced by the prevalence of urinary incontinence, pelvic organ prolapse (POP), abdominal muscle separation and pain that are experienced by female runners after having a baby. Urinary incontinence and POP can result from the stress that is place on the pelvic floor muscles. For a review of the anatomy of the pelvic floor muscles click 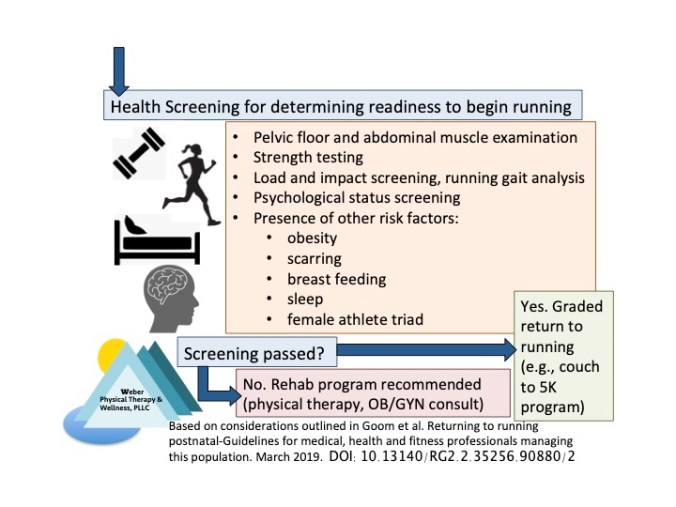 The screening process is recommended to cover the following:
The screening process is recommended to cover the following:
