In the United States, almost 1 million knee replacements are performed each year. That number is expected to continue increasing through 2030. Simply put, knee replacements are becoming common place.
But is a knee replacement the right thing for you? If so, when?
A recently published study out of Northwestern University’s School of Medicine in Chicago indicates that the timing of a knee replacement is absolutely crucial for success (Ghomrawi et al. 2020). Of patients in the study who could benefit from knee replacement, 91% waited too long. On the flip side, 26% of patients who didn’t need a knee replacement, underwent the surgery anyway.
What indicates that someone has waited too long to have a knee replacement?
They lose the ability to walk and move around well. As a result, they become more sedentary. Sedentary people develop cardiovascular and other health issues. With a decline in overall health and the ability to engage in life’s activities, depression tends to creep in as well. When someone goes into knee surgery in poor physical health, rehabilitation is more challenging and the outcome is subpar. Walking and moving around are still difficult—even after the knee replacement.
What happens when someone has a knee replacement too early?
A person has a major surgery, taking risk unnecessarily. They may also need to have another knee surgery in the future. And the second surgery will likely be more challenging than the original surgery.
When is the right time to have a knee replacement?
Surgeons are developing more strict criteria for deciding who should pursue knee replacement. Multiple factors are taken into consideration including: pain, joint function, age and X-ray assessment. Xray assessment should show absence or near absence of cartilage in at least one compartment of the knee. In other words, significant degenerative joint disease.
Another factor, is the patient’s expectations. If pain levels are low to moderate a patient is less likely to appreciate a new knee as much as if their pain levels have been relatively high. The more drastic the reduction in symptoms, the greater positivity the patient will have mentally and physically.
If you are not quite ready to have a knee replacement, but are beginning to lose your ability to walk and move around well, consider consulting a physical therapist. Strengthening the muscles around the knee with specific exercises can sometimes go a long way in increasing function and putting off that knee surgery to a time when it is appropriate and most beneficial. And after you finally do have that knee replacement, your physical therapist would love to assist you in maximizing your mobility and strength.
Reference:
Ghomrawi et al. 2020. Examining the timeliness of total knee replacement among patients with knee osteoarthritis in the U.S. The journal of Bone and Joint Surgery. 102(6):468: 10.2106/JBJS.19.00432
The beauty of making your own snack bars is that you can control all of the ingredients that go into them. Many of the commercially available protein and energy bars have very high amounts of sugar. While they are marketed as health foods, they are no better than any candy bar. For that reason, I find it worth-while to make my own.
Ingredients:
2 cups of old-fashioned oats
1 cup of chia seeds
1 cup of raw pumpkin seeds (shelled)
1 cup of raw Sunflower kernals
1 cup of dried cranberries
4 tbsp of coconut oil
1/3 cup of 100% maple syrup (Grade A)
1/3 cup of almond butter ( I recommend Barney Butter with no sugar added)
Instructions:
Combine the oats, chia seeds, pumpkin seeds and sunflower kernals.
Spread mixture onto a cookie sheet and roast for 15 minutes in an oven that has been pre heated to 350 F.
Place the coconut oil, almond butter and syrup in a small pot. Heat and stir constantly over medium heat until all ingredients are melted and well mixed. Pour over the roasted oat and seed mixture, add dried cranberries. Mix all ingredients until well coated.
Pack ingredients into a 9-inch X 9-inch or similarly sized pan. Refrigerate 2-3 hours until they are set. Cut into 16 bars and serve. Bars will keep for several weeks in an airtight container.
***
Fun facts about seeds and why you should eat them:
Chia seeds: contain more calcium than a serving of milk. They also contain high amounts of antioxidants, fiber, iron, and omega 3 fatty acids which fight inflammation and raise HDL (“good cholesterol”).
Pumpkin seeds: contain several minerals which are important for thousands of chemical reactions in your body including, magnesium, zinc, copper, iron, manganese and phosphorus. They are also high in vitamin K which is important for blood clotting and bone health.
Sunflower kernals: contain several minerals and vitamins that are needed for thousands of chemical reactions in the body that support metabolism and the immune system function. These vitamins and minerals include selenium (good for thyroid health), iron, folate, pantothenic acid, magnesium, manganese, copper, vitamin B6, vitamin E, niacin, and zinc.
“Somedays it takes me about 45 minutes to get on a pair of briefs”, said one of my patients with Parkinson’s Disease (PD).
As a physical therapist, I knew that we had to solve this problem. Spending 45 minutes of life donning clothing is no way to live.
If you are reading this and have PD, you may know what I am talking about. For those of you who are not as familiar with PD, this is a small window into the world of living with PD.
And when the problem of donning clothes reaches this level, it significantly reduces quality of life. It is not only the frustration that the patient with PD experiences, but the further drain on his or her already limited energy.
Without exception, the number one complaint I get from all of my patients with Parkinson’s Disease is fatigue. To those of us living outside of the PD world, we might think that the tremors and mobility impairments are the number one complaint—and they are a big deal. But the fatigue component trumps them all. Why? Because fatigue means that one can spend less time in life enjoying the company of others and engaging in activities that bring him or her joy and purpose.
Why can it be so hard to get briefs on when one has PD?
Stiffness and rigidity: PD causes stiffness and rigidity throughout the body, particularly in the spine and hips. This can make it difficult and/or painful to bend forward towards the feet or bring a knee up to lift a foot through the leg hole of a pair of briefs.
Motor initiation, planning, and sequencing: With PD, some of the tasks that one used to take for granted and didn’t even think about (i.e., putting on clothes, getting out of a chair) become very difficult. Sometimes getting the tasks started is the hardest part. And when a task involves a series of steps, such as putting on briefs (i.e., orienting the briefs properly, getting legs into the right holes), becomes very difficult.
Reduced amplitude of movement: Typically, once we learn how to do a motor tasks in our lives, we have an automatic program in our brain as to how much effort or force is needed to accomplish the task. For instance, getting into and out of a chair is easy because the brain “knows’ how much force should be put through the legs to rise from the chair. If the chair is exceptionally low, the brain knows that more force is needed through the legs vs. if the chair is a higher. With PD, people lose that sense of calibration and not enough effort/force is put into the movement and the task is not accomplished. Most of my patients come to physical therapy with complaints of falling back into a chair when they try to come to standing. Their brains have recalibrated the motor program for getting out of a chair. This recalibration occurs across all movements including fine motor skills, that are needed to handle a pair of briefs and orient them properly for donning.
Tremors: Tremors that are characteristic of PD obviously hinder motor tasks—especially fine motor tasks that take precise grip to open up and orient a pair of briefs for donning. And when a task becomes more difficult, people with PD often experience worsened tremors.
So what can a physical therapist do for a patient with PD who cannot get his briefs on? It depends on the individual’s characteristics, but what follows is an outline of the approach that I take:
Determine the patient’s primary limitations in putting on briefs. Some people exhibit stiffness and rigidity as their primary issue. If this is the case, we spend time working on mobility and stretching to regain range of motion in the spine, hips and other lower extremity joints. We make sure the motions of putting on briefs are possible. For other people, they have the available range of motion needed to put on briefs, but they are not putting enough effort or force in to make the task possible. For example, they cannot lift their foot high enough to get it into the leg hole on the briefs. For other people, it’s the fine motor skills that are the biggest limiting factor. Sometimes getting the briefs opened up and properly positioned to facilitate donning is the biggest problem. And sometimes, it’s a combination of all of these issues.
Design a rehab program that targets the biggest limitations and practices the skill of putting on briefs. More than likely, there is combination of limitations described above that need to be addressed. A comprehensive program might work on fine motor skills with one’s hands, mobility and flexibility and recalibration of force needed to accomplish the task of putting on briefs. For the latter, LSVT-BIG exercise is a well- researched exercise program that works very well for retraining the brain to initiate movements with greater force to make everyday tasks possible. LSVT-BIG is backed by over 25 years of U.S. National Institutes of Health research as being effective and can have long-lasting effects post physical therapy treatment. Weber Physical Therapy and Wellness is one of the only physical therapists in Southeast Idaho to offer LSVT-BIG treatment.
Take comorbidities into consideration that complicate one’s life with PD. In the life of someone with PD, PD often takes center stage. However, other health issues layered on top, may make things even more difficult. To maximize the benefit from physical therapy, these other problems need to be taken into consideration. For instance, it is common for people with PD to struggle with dementia, visual deficits, other orthopedic injuries/pain that exacerbate the issues that they already stem from having PD.
The patient quoted at the top of this article had a unique presentation in that it was actually his comorbidities that were limiting his ability to don his briefs. He saw double up close and had dementia that caused him to hallucinate at times. He had some motor planning deficits that would get him “trapped” in a position, bent over with the brief only around the tips of his toes. And that is where he would stay for 35 minutes. And that was after the 10 minutes it would take him to fiddle with the briefs to open them up and find the leg holes—seeing double makes this very difficult. As a physical therapist, I cannot fix someone’s vision, but I can adapt a task so that it might get around some of the problem.
I built this patient a dressing aid that holds his briefs open for him so he can easily see the leg holes. And since the device holds the briefs open, he doesn’t have to hold onto them and can focus on just getting his legs into the leg holes. Once his feet are in place, he just has to grab the waist band and pull up. That’s it.
This device allows him to get his briefs on in 3 minutes or less. Saving him 42 minutes to do things that he loves and make his life full.
Adaptive device for donning briefs, constructed for a patient with Parkinson’s Disease.
Adaptive Device holds briefs open, making it easier for a patient with Parkinson’s Disease to put them on.
If this story sounds similar to your situation or that of someone you love, consider physical therapy. As a physical therapist I provide tailored, one-on-one services for patient driven success. You can ‘wear the pants’ again.
***
Carolyn F Weber, DPT, PhD is one of the only physical therapists in Southeast Idaho who is certified in LSVT-BIG treatment for Parkinson’s Disease. She provides one-on-one physical therapy and fitness programming for clients with Parkinson’s Disease in the comfort of their homes. Medicare of Idaho and Railroad Medicare insurances are accepted. You do not need a doctor’s referral to get started—just call or email Carolyn to set up your first appointment.
Carolyn also leads an exercise group on Wednesday’s at 5 PM at the River of Life Church located at 1211 S 5th Ave, Pocatello, Idaho 83201. This class is FREE, but space is limited. Email Carolyn for more information or to her know that you want to reserve your space in the class.
I am a hard-core introvert. I not only enjoy solitude, I revel in it. I love my work as a physical therapist, connecting with people, getting them back on their feet and helping them discover their potential. But outside of work, there is nothing like quiet time. On a run, on my bike, alone at my desk with my thoughts…. In fact, outside of work, I am almost ashamed to admit that the need to social distance during the pandemic, didn’t bother me much at all.
But I am far from anti-social. There is nothing I value more than connecting deeply with those I hold close to me. When I sit down at the table with someone, let’s pass up the conversational appetizers on celebrity twitter accounts and someone’s new eyebrow tattoos. I don’t care. Let’s get to the main course please. Like let’s talk about what rocks your world to the core, where you see yourself in 5 years, what your life’s mission is.
Someone once asked me what my most valued possession is. I said “time”. Time to spend wisely with people whose passions run deep and aren’t afraid to chew on an issue for a while with you. People who will share in your journey, listen to your best and worst ideas and kick your ass when you need it most.
I was accused by this Someone as being “deep”. Like it is a bad thing.
This is all to say that, I have had few experiences in my life when my soul has felt nourished… by people I felt were totally part of my tribe.
One of those few experiences was 9 years ago when I attended a Women’s Running Camp at Active at Altitude in Estes Park Colorado. This Camp is the genius of Terry Chiplin who moved to the U.S. from England with his wife Jacqueline to make highest runner’s high possible in the Rocky Mountains.
Running the trails of Rocky Mountain National Park with fellow Active at Altitude Campers in 2016.
Running camp includes several days of living in the Chiplins’ home with other campers, amazing food to fuel your running, running on the best trails that the Rockies have to offer, learning about injury prevention, training and the best part….comaraderie and developing a game-changing mindset.
They not only host Women’s Running Camps at three different levels (Beginning, intermediate and Advanced), they also host a Co-Ed Trail Running Camp—one in the spring and one in the fall. For complete information on the Camps, visit the Active at Altitude website.
Pre-run fun with fellow Active at Altitude Campers in 2016.
The entirety of the camp was invaluable, but the mindset piece was absolutely game changing for me and took me from running enthusiast to running the Boston Marathon and tackling challenging mountain races that I never dreamed of running. And meeting people who wanted to talk about all of those deep things on a run or in between was so amazing and therapeutic. I felt like I had finally arrived—this was the tribe I was missing my whole life! And this year—in 2021—- in a world that changes minute-to-minute, what is deep in us, our need to connect—our need to find our tribe doesn’t change. Especially after 2020, this type of experience may be exactly what you are craving. And this is why I am so excited to be returning to trail Running Camp in Fall 2021!
For those of you who have piqued interest, my complete reflections on my Camp experiences were captured in my conversation with Chiplin back 2016. I can’t say anything different or better today. An excerpt of this conversation follows.
**
Chiplin: Can you tell us something about your running history prior to 2012?
Me: As a kid, I played a lot of team sports in which running was a punishment, so it wasn’t until college and graduate school that I took up running as a form of exercise and found that I enjoyed it. A friend convinced me to run a half marathon, my first race ever, in 2005. Between then and 2012, I ran several 5Ks, 10Ks and a few more half marathons. My race times were improving and I began to take running more seriously. I especially got a lot of enjoyment out of running after moving to New Mexico in 2009 and then Idaho in 2011 for professional reasons, as these regions introduced me to running at higher altitudes and I got my first tastes of trail running. However, I felt that my running had plateaued and, perhaps oddly, I didn’t truly feel like I could call myself a runner. In 2012, I felt like I needed something to bust down the wall that was preventing me from improving and I was also beginning to feel a bit beat up physically. Never having had any formal coaching, I suspected that my form was pretty inefficient and I wasn’t taking the right approach to training—at least one that worked for me. Although I couldn’t really articulate it at the time, I also felt that I wasn’t fully experiencing all that the sport had to offer. That’s pretty much what brought me to Active at Altitude in 2012.
Chiplin: You came to one of our Women’s Running Camps in 2012. What was your experience like?
Me: The Women’s Running Camp was exactly what I needed to elevate my running from the plateau that I had reached physically—but also mentally, which was a life-changing discovery for me.I came to camp mostly expecting to figure out what I needed to do differently to better approach the physical aspects of running—and there was certainly that! Through a video analysis I saw for myself that I was a profound heel-striker and had lots to work on there and I learned a tremendous amount about running work outs, cross training and proper nutrition, among other things. However, the real watershed moment for me at the Camp was discovering how far I needed to come mentally and that I would never become a runner if I didn’t first believe that myself! I was always told in high school that I was a terrible runner, but team sport coaches left it at that and never provided constructive criticism. During camp, I came to the realization that I had been letting other people’s criticisms define me and my potential even though I am a pretty independent person in most everything I do and I think I am fairly strong mentally. But I really realized that I could be stronger with a supportive network of people with whom I could safely share my aspirations for running—or anything in life….a network of people that provide a safe environment to dream big and serve as a sounding board. The Women’s Running Camp provided that network. To this day, I have stayed in contact with fellow campers from the 2012. This supportive atmosphere and community established by the Camp is a primary reason that I also came to Women’s Running Camps held in 2013 and 2014 as well as Trail Running Camp this year. The Camps also take place in an absolutely stunningly beautiful area of the country and provide a wonderful place to run with like-minded folks. The hospitality at Active at Altitude is amazing and meal times are always a highlight—they are really fun and provide great venues for laughing, dreaming, planning, mental training…they provide food for the soul as much as they do for the body.
Chiplin: What was your biggest take away from that camp?
Me: I think the biggest take away from Camp was a new mental foundation on which to build myself as a runner—or anything–as well as a new framework for living life. After Camp, I knew that I wanted to achieve new goals, but that the focus should really be primarily on the journey towards reaching those goals and that living life with gratitude was paramount. I also learned the power of visualization as a tool in realizing goals. Camp was my first real immersion in making mind-body connections and I was absolutely blown away. In 2014, I ran a personal best at the Missoula Half Marathon. At the time, I knew it was a bit lofty, but doable to run the race in 95 minutes. I did the math and knew what pace I had to hit. I had never run the course before, but had a map and course profile. Using only those three pieces of information, I visualized several times before race morning what it would feel like to run the race in 95 minutes—with gratitude for every step. I ended up finishing in 1:35:06 and almost couldn’t believe it.
Chiplin: You formed a close bond with your bunkroom buddies. What was special about this for you?
Me: Yes. My bunkroom buddies almost couldn’t have been more different than me in many ways—age, profession, ethnic background, religion, physical appearance…everything. But we were all united at Camp in the act of self-discovery and redefining ourselves as people. I have remained in contact with Mirabelle Tinio, one of my bunkroom buddies, who continues to be a fountain of inspiration in her dare to dream big back in 2012 and run with the Canadian Mountain Running Team—a goal that she once didn’t think was possible, but that she accomplished. Mirabelle represents boundless energy packaged in a frame that is just over 5 feet tall. At about nine inches taller, I have fond memories of she and I running the streets of Boulder, CO—we had a good laugh after I told her that we must look a bit like Penn and Teller to those we were passing by! In the last four years, I’ve only had a chance to see Mirabelle twice, but she remains a key person in my support network. Interacting with Mirabelle and others at the Camp made me realize that in today’s world, people tend to focus too much on what makes us different with respect to so many things– ethnicity, religion, gender, physical appearance, etc.—but we are all human beings—we all cry, sweat and bleed. We all have fears and doubts. We all also dream and have a tremendous amount of potential–more than we usually realize–to make those dreams a reality. Mirabelle is living, walking … running proof of that. With an environment created by a supportive network of people in which it is safe to dream and safe to take risks, we can accomplish what may have once seemed impossible.
Front row: Me and Mirabelle Tinio, taller and shorter … total opposites united in passion for running—with Active at Altitude Campers in 2016 (Co-ed Trail Running Camp).
Chiplin: Since camp you have also qualified for Boston twice. How important was your camp experience to helping you achieve this and what was your highlight from running Boston?
Me: Running a marathon, let alone qualifying for Boston, wouldn’t have been possible prior to coming to Camp—physically, but particularly mentally. During the Camp, I learned that I didn’t have to listen to the doubts and fears of others about something that I could and would do. While I was training for my first marathon in 2013, a coworker had learned what I was doing and said to me one day, “running a marathon is a really good goal to have even if you don’t finish it”. I learned that people commonly project these criticisms onto others, but they are really just the reservations that they have about themselves. My coworker was rudely surprised when I not only completed the marathon, but also qualified for Boston, undercutting the qualifying time by nearly 10 minutes.
After Camp, consciously running with a sense of gratitude became a practice for me that got me through the marathon. Before race day, I made a list of people that I was grateful for and, up until the last 5k of the race, I had this mental playlist of people and fond memories associated with them that I was flipping through. I dedicated the last 5k of the race to every person who ever cast a shadow of doubt on my running ability—turning their negativity in motivation to cross the finish. When I started the race that day, my goal had been to simply finish it; although the Boston qualification time was in the back of my head, it definitely wasn’t a focus. To BQ was just the frosting on the cake.
Boston 2015 was great, but 2014 will always have a special place in my heart. I was really nervous, of course, to run Boston as my second marathon ever, but it was also the year after the horrific bombings of 2013. I remember being at the Salt Lake City airport and when I arrived at the gate for the flight to Boston it was this sea of really fit people wearing the Boston jackets from years’ past and I instantly got really anxious. I started having a bunch of negative self talk run through my head—wondering if I was really worthy of running with seasoned Boston Marathoners, etc. I actually stepped away from the gate at one point. When I came back, a woman in her 60’s struck up a conversation with me and asked me if I was running. She explained to me that she had run Boston several years in a row and had planned 2013 to be her last go at it —she had had every intention of hanging up her shoes after running in 2013. But she said that after the bombing, she would absolutely not do that and that she needed to be part of the 2014 race that would take back the City and show people that we wouldn’t live in fear—that we must overcome. At this point, I realized that this was way more than a race and finish times. Boston represented so much more—it was all about overcoming. Another key moment in the race was during the latter half. We were running up hill and I was feeling less than fresh when some guy in the crowd shouted “Meb won! An American has won!” Those of us who were feeling the burn were instantly reenergized. It was amazing. Since Boston 2014, I have thought very differently about running. There’s always competition, but mostly running is about overcoming—it’s about the journey. It doesn’t matter how fast one is, but every one who toes the start line of any race had to overcome something to get there. Toeing the start line is a victory and crossing the finish is the celebration of a fantastic journey of overcoming.
We’ve already arrived at the third Sunday in January. Right around this day, give or take, is when most people quit working on their New Year’s Resolutions. Some people now call this Quitter’s Day.
Quitter’s Day was “discovered” back in 2019, by Strava. Many of you may use or know of Strava as an exercise tracker.
The problem with New Year’s Resolutions
I am a dreamer. Dreaming is what brings me some of my best (and worst!) ideas. People seem to get better at dreaming as a year comes to a close and they reflect on the past year. Some of these dreams turn into something that sounds more realistic—-New Year’s Resolutions.
But Resolutions, dreams, goals—whatever you want to call them, remain as such, unless we have the right plan. And HOW we plan to achieve our resolutions is the key in pushing right past Quitter’s Day.
“A goal without a plan, is just a wish”
— Antoine de Saint-Exupéry
The key to achieving a big hairy audacious goal (a.k.a. BHAG), especially when it revolves around health and wellness, is to establish a plan that implements small changes in your daily life. And when I mean small …. I mean small.
Plan=Establishing Tiny Habits
BJ Fogg, PhD of Stanford University has written a book called Tiny Habits: The Small Changes that Change Everythingwhich outlines how to go about making small changes in your life that lead to lasting habits. And lasting habits can lead you to your BHAG.
Dr. Fogg discusses what he calls “Motivation Waves”. As all of you have experienced, motivation fluctuates across the month, a day, an hour within a day—unfortunately. Simply put, when motivation is high, it’s possible to do hard things such as a two-hour training ride or run. When motivation is low, doing any form of exercise for two hours can seem impossible.
BJ Fogg, PhD explains Motivation Waves
In short, it’s not recommended to set a New Year’s Resolution of working out 2 hours per day, especially if that is a drastic change from your current habits. And all of us experience motivation waves to some extent.
In a recent interview, Mark Hyman, MD and BJ Fogg, PhD, discuss the book Tiny Habits: The Small Changes that Change Everything. Dr. Hyman talks about how tiny habits absolutely changed his health and wellness routine. Dr. Hyman tells the story of how he had a long-time dislike of strength training, as it was just something that he didn’t enjoy. He thought strength training was “hard” and “uncomfortable”. His motivation for strength training was low, even though he knows as a physician that it is a really beneficial thing for fighting sarcopenia (muscle loss with aging). But Dr. Hyman was able to change his habits and he relays the story of how he started with doing one push up per day. Yes—one. And he did that pushup while he waited for the shower to warm up. Instead of standing there waiting for water temperature to increase, he would get down on the ground and do one push up. Eventually, that one pushup became easier. Several years later, he hired a personal trainer and now engages in regular strength training. A tiny habit turned into positive behavior change that will greatly benefit his health in the long term.
To hear the complete interview on the Doctor’s Farmacy podcast, click here.
To hear more about behavior change from BJ Fogg, PhD, click here.
Tiny Habits have worked for Me!
I also know from first-hand experience, that implementing long lasting change, requires incremental changes over time. When I first began “distance running” as a form of exercise in my late teens, running a mile was hard. I would run down my parents’ street and then back to the drive way—that was it.
But as I got better at running one mile, I became curious. How far could I go? Little by little, I worked my way up to 2 miles and eventually ran my first half marathon 6 years later. That’s right —-6 years later. I started low and I went slow. And then 15 years later, I became a Boston Marathoner. If you’d have asked me in 1999 whether or not I’d ever want to run a marathon—much less be able to—I would have said “hell no”.
Weber running the 2014 Boston Marathon–15 years after she began running–only 1 mile at a time.
Moral of the Story? Don’t say “hell no”. Start low and go slow.
If you want to read a really inspiring story of someone who has implemented small changes everyday to become the first person with Down’s Syndrome to complete an Ironman Triathlon, read Chris Nikic’s story on his website here. Learn his life changing method of “1% better”.
My exercise prescription for patients: Start low, go slow
This is the underlying principle for how I prescribe exercise for the majority of my patients—especially those with a long-time history of difficulty with lifestyle change. An example of this is a patient I just saw last week who barely averages 1000 to 2000 steps per day. My recommendation to him? Over the next month, let’s see if we can get your daily step count to 2,500 steps per day. If one were to increase his step count from 2000 to 2500 over 4 weeks, that means increasing step count by 17.8 steps per day. One could easily take 17.8 steps by parking the car 5 parking spaces further from the grocery store entrance than they normally do. A small change that can be built into everyday activities.
Dream big, but start low and go slow. Above all else—don’t quit.
“Fall” is a four-letter word, in more ways than one, especially as people enter their later years. Most of my older patients know full well that falls can be associated with broken bones and quick decline. Most of my patients over 70 have some kind of loss of what is commonly referred to as “balance” and this is exacerbated by Parkinson’s Disease. Balance is one of those things we take for granted until we realize that it is becoming compromised. The lyrics by Tom Keifer (performed by Cinderella) sum it up pretty well in that regarding balance you “don’t know what you got ‘till it’s gone”.
Balance is often talked about as one thing, but it’s actually pretty complicated. To simplify things a bit, your overall ability to maintain your balance (i.e., stay standing upright) is dependent on how well three major things in your body are functioning:
vestibular system. The vestibular system is located in your inner ear and sends signals to your brain about motion, head position and spatial orientation. The brain integrates all of this information and then sends signals to the rest of the body to stabilize our head while we move and maintain posture so we don’t fall down.
somatosensory system. There are specialized structures located throughout your body that tell the brain where your joints (e.g., knees, hips, ankles) are in space and allow you to feel textures, pressure and temperature on the surface of your skin. As we will discuss, the working ability of sensory receptors in the soles of your feet play an especially important role in balance because they literally allow your brain to feel what you are walking on and where they are in space.
visual system. Your eye sight is important for seeing where you are in space and for telling your brain what may exist in your environment that could challenge your ability to stay upright (e.g., slick surfaces, rocks to step over, stairs).
For more information on the vestibular system:
Your brain is able to integrate signals from the three major systems listed above and then send signals to your muscles (also known as motor output) to adjust your posture, take a step, tilt your head—whatever you need to do to prevent yourself from falling. This obviously happens very quickly—in a tiny fraction of a second—when working optimally. For most of our lives this happens without us even thinking about it.
However, as we age, so does our vestibular, visual and somatosensory systems, and they don’t work quite as well as they used to. When the systems that control our balance begin to decline, our ability to navigate environments we once used to, such as curbs and bumpy sidewalks, becomes compromised. Balance is also affected by a person’s mindset, fatigue/attentional capacity, muscle coordination and integrity of the skeletal system. If you are distracted by someone shouting hello to you or you have lasting effects of injury (limited joint mobility), these are going to further challenge you balance. Furthermore, when you superimpose disease, such as Parkinson’s Disease, on top of an aging visual, vestibular, and somatosensory system, one’s ability to maintain upright posture—or prevent falls—-becomes even more compromised.
Although commonly known for its association with advancing type 2 diabetes, peripheral neuropathy has also been noted to be common in people with Parkinson’s Disease (Viseux et al. 2020). Peripheral neuropathy is characterized by poorly functioning nerve fibers in the soles of the feet that transmit information to the brain, allowing one to experience touch, position in space (proprioception), vibration, pain and temperature. The transmission of this information to the brain is critical to maintaining your balance and avoiding stepping in places that may cause injury. Romagnolo et al. (2018) estimates that 55-75% of patients with Parkinson’s Disease who are treated with levodopa (by oral or intestinal infusion) could develop peripheral neuropathy. The reason for developing peripheral neuropathy is unclear and it may also be linked with vitamin B12 deficiency and/or degradation of nerve fibers in feet and other parts of the body.
So the question is, how can we best prevent falls for people with Parkinson’s Disease?
Improving balance requires a multi-faceted approach. Central to this approach is working with a physical therapist to improve strength and ability to use the visual, somatosensory and vestibular systems together to the best of your abilities. A physical therapist can provide a safe environment in which one’s balance can be challenged, but injury can be avoided. Optimizing balance also includes a checkup on the three major systems that contribute to balance. This includes making sure that one is doing everything he or she can to preserve the health of one’s eyes and improve eyesight to the greatest extent possible. Has a person been putting off dealing with cataracts? Now may be the time. How is the health of the vestibular system and ears? Believe it or not, a buildup of wax in your ears can interfere with balance. Other more serious problems such as vertigo, Meniere’s Disease, acoustic neuroma, and vestibular neuritis can also interfere with your vestibular system. If you suspect or know that these are problems, then you need to see an ENT (Ears Nose and Throat specialist), neurologist and may even be referred to a physical therapist depending on the root of the problem. Another piece of the approach is making sure that one is maximizing the sensory information coming up to the brain from their feet to better inform the brain about where the feet are in space and what kind of surface they are standing on. And this is the best news: recent research has shown that increasing the sensory stimulus to the feet can enhance motor control for improved balance (Viseux et al. 2020).
Sensory stimulus to the feet can be enhanced through the use of textured insoles.
Research recently reviewed by Viseux et al. (2020) indicates that textured insoles can help not only people with Parkinson’s Disease improve their walking and balance, but also people with multiple sclerosis and healthy people too. Wearing textured insoles has been found in studies to decrease body sway from right to left (Qui et al. 2013; Robb and Kelley, 2000), improve postural stability even with eyes closed or standing on foam surfaces (Qui et al. 2013), increase step length (Qui et al. 2013), decrease the number of steps needed to complete a 180 degree turn (Robb and Kelley, 2000), improve functional reach tests (Volpe et al. 2017), improve single leg stance time and muscle activation in the lower leg (Jenkins et al. 2009) and improve ability to feel the bottom of the foot (Lirani-Silva et al. 2017).
How quickly are results achieved after wearing the insoles? Studies used different time frames for testing, but improvements in two studies were noted immediately (Jenkins et al. 2009; Qui et al. 2013).
What’s more is that data indicates that long-term use of insoles may promote increased representation of the bottom of the foot in the primary somatosensory cortex of the brain which improves ability to feel the bottom of the foot (Qui et al. 2013).
Where can you get such insoles? Below is a listing of some examples. As a disclaimer, I have no financial connection with any of these companies and I am not necessarily promoting their products—I am merely providing examples:
If you are wondering about the specific details of the research studies examining the effects of wearing textured insoles on balance and walking, please see brief summaries below:
Qui et al. 2013:
Participants: 20 healthy people and 20 people with Parkinson’s Disease
What was done in the study: Participants stood on firm and foam surfaces while barefoot, wearing smooth insoles, and while wearing textured insoles. While doing this, standing balance was measured using a force plate. Specifically, the data included measures of anterior -posterior and medial lateral sway.
Results: Only the textured insoles decreased medial-lateral sway in the Parkinson’s group on firm and foam surfaces.
Robb and Kelley 2020:
Participants: 7 people
What was done in the study: The dynamic stability of participants was examined wearing footwear only, footwear with a textured insoles or footwear with a nontextured insoles. Measurements were collected at the beginning of the study, 4 weeks later and 5 weeks later.
Results: Improved dynamic stability was noted in the frontal plane and the number of steps required to make a 180-degree turn was reduced in those wearing the textured insoles.
Volpe et al. 2017:
Participants: 20 people with Parkinson’s Disease
What was done in the study: All participants performed balance training for two weeks (5 days per week). Half of the participants wore textured insoles. Measurements on functional reach testing was completed at the beginning of the study, immediately following the 2-week balance training program and 4 weeks after the balance training ended.
Results: People who wore the textured insoles had improved functional reach tests even after the balance training program had ended.
Jenkins et al. 2009:
Participants: 40 people with Parkinson’s Disease and 40 age-matched healthy controls
What was done in the study: Study participants wore ribbed insoles (these are insoles with a ridge around the border of the insole) and regular insoles during separate walking trials. Single leg stance time was measured while walking as well as electromyography measurements of lower leg muscles.
Results: wearing ribbed insoles improved single leg stance time during walking and anterior tibialis activation was improved according to EMG measurements.
Lirani -Silva et al. 2017:
Participants: 19 participants with Parkinson’s Disease
What was done in the study: At the start of the study, sensation in the bottom of the participants’ feet was tested using Semmes-Weinstein monofilaments. At the start of the study, all participants had their walking filmed for stride length measurements. All participants wore textured insoles for 1 week and the same measurements were taken again. Participants were instructed to wear regular insoles for the week following the study. After the week following the study, a third set of measurements was collected.
Results: After one week of wearing textured insoles, stride length and sensation in the soles of feet were improved. After one week of wearing regular insoles (following the one week with textured insoles), plantar sensation improvements were still present, but walking improvements were not. Study authors concluded that continuous use of insoles may be needed to improve gait.
References:
Jenkins et al. 2009. Plantar cutaneous sensory stimulation improves single limb support time, and EMG activation patterns among individuals with Parkinson’s Disease. Parkinsonism and Related Disorders. 15:697-702.
Lirani- Silva et al. 2017. Continuous use of textured insole improved plantar sensation and stride length of people with Parkinson’s Disease: A pilot study. Gait and Posture. 58: 495-497.
Qui et al. 2013. Effects of textured insoles on balance in people with Parkinson’s Disease. PLoS. ONE: 8(12). e83309.
Robb and Perry. 2020. Textured foot orthotics on dynamic stability and turning performance in Parkinson’s Disease. Journal of Motor Behavior. 52: 396-403.
Romagnolo et al. 2018. Levodopa-induced neuropathy: a systematic review. Movement Disorders Clinical Practice. 6:96-103.
Viseux et al. 2020. Postural instability in Parkinson’s Disease: Review and bottom-up rehabilitative approaches. Clinical Neurophysiology. 50: 479-487.
Volpe et al. 2017. Effects of a sensory-motor orthotic on postural instability rehabilitation in Parkinson’s Disease: a pilot study. Journal of Clinical Movement Disorders. 4:11.
Masks, fear, illness, death, economic shutdown, hoarding and empty grocery store shelves. These things are forever etched in the history books of 2020 in association with the COVID19 pandemic. Pre-pandemic, most Americans were fortunate enough to have never experienced any problem with food supply and took fully stocked grocery stores for granted. However, for years, food production and distribution processes have been vulnerable to breakdown in the face of environmental, economic and sociopolitical crisis. The COVID19 pandemic has merely illuminated this. But the problem runs deeper than simply not having the grocery store shelves fully stocked. Even when contemporary food production and distribution processes are running smoothly, they produce foods that have diminished nutritional value by the time they get to the grocery store shelves. And it gets worse every year. To put it simply, the broccoli in today’s produce section has less nutritional value than the broccoli of 5 years ago. The declining nutritional value of our food has been a key driver of the rise of illness resulting from metabolic disorders in the United States. And those with metabolic disorders have weakened immune systems and are more prone to illness such as COVID19. All of the processes associated with production, distribution and waste management, otherwise known as our “food system” is intimately intertwined with human health.
And the intimate relationship between our food system and human health is exactly why I care about this as a physical therapist. Lack of access to healthy foods lowers the potential for all of us to lead active and healthy lives. Poor nutrition is even the root cause of why people end up in physical therapy in the first place. I spend part of my time as a physical therapist working at a skilled nursing facility. We frequently receive patients from hospitals that have been diagnosed with metabolic encephalopathy, which alters ones mental state. The cause of metabolic encephalopathy is often liver disease, uncontrolled diabetes and kidney disease, which for many people is preventable with good nutrition. Poor nutrition also increases the risk of infection and often our metabolic encephalopathy patients come in after they’ve suffered a urinary tract infection. While these types of metabolic encephalopathy are reversible with overcoming infection and getting metabolism back in check, these people spend weeks in recovery and develop severe weakness and difficulty with daily activities (i.e., walking, getting out of a chair). This health decline often results in significant loss of quality of life and for some causes them to lose their ability to live independently. Furthermore, lack of access to good nutrition is especially problematic for people overcoming injury or coping with chronic illness. The outcomes that I can help my patients achieve through physical therapy interventions (i.e., increased strength, endurance, mobility, decreased pain) are diminished when they don’t have access to healthy foods that complement their physical rehabilitation. The role of nutrition in our physical well-being is not to be underestimated.
COVID19 has monopolized the news in terms of illness and death rates, for obvious reasons, but it is interesting to put some facts and figures into perspective. About 50% of Americans have diabetes or are pre-diabetic and 530,000 people die annually in the U.S. due to poor nutrition, which is almost 1500 deaths per day (Dr. Mark Hyman podcast: What does food have to do with COVID19?). By comparison, about 265,000 people have died from COVID19 in the US so far this year, with only about 1 month left in the year. This is absolutely not to diminish the gravity of the COVID19 situation or diminish the value of the lives that have been lost due to it. However, it is important to point out the magnitude of the nutrition problem in the U.S. Most perceive that malnutrition is a problem that is restricted to 3rd world countries. Not so. What’s more is that poor nutrition and COVID19 have an important linkage. People who are more vulnerable to COVID19 infection and subsequent death are those that are “metabolically compromised”. Good nutrition is necessary to have a strong immune system to fight of infection of any kind—including COVID19. Specifically, one might consider zinc, vitamin A and vitamin C which are critical, among other nutrients/vitamins, for a strong immune system and nearly 40% of Americans are not getting adequate daily intake of these. The short story is that our resilience against death from COVID19 or any infection could be drastically improved through good nutrition that supports our immune system. Should I mention at this point that 60% of your immune system resides in your gut? Hyman podcast: What does food have to do with COVID19?) Yep. That means the quality of the food you eat is of utmost importance.
OUR VULNERBLE FOOD SYSTEM AND HOW IT IS COMPROMISING OUR HEALTH
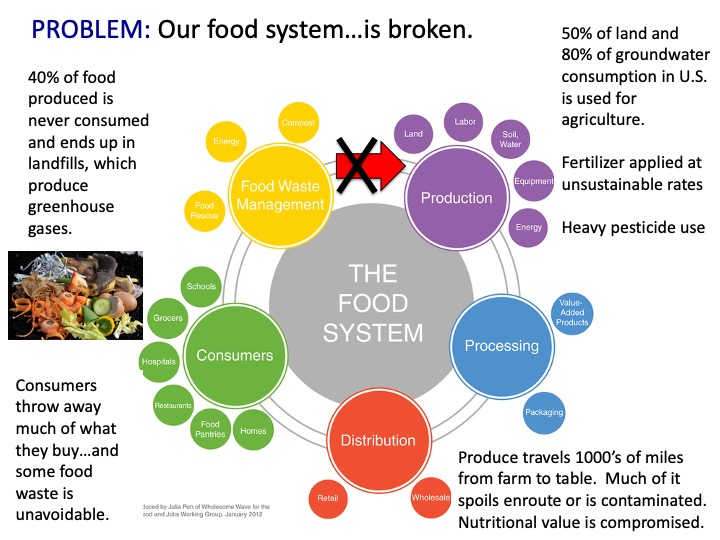
To illustrate why food insecurity exists as well as the relationship between the food system and human health, let’s examine the three major parts of our food system and their vulnerabilities to environmental, economic and sociopolitical crises:
Food Production/Processing: In the United States, food production utilizes 50% of land and 80% of the total freshwater that is consumed (Gunders, 2012). This rate of water usage is faster than aquifer recharge in some regions (Sachs 2015). Food production also depends heavily on fertilizer and pesticide application, which is adversely impacting ecosystem biodiversity (Sachs, 2015). Additionally, farming is increasingly focused on the mass production of fewer staple crops (i.e., wheat, corn and soy). Reduced crop diversity reduces the nutritional value of the average diet and makes food production less resilient to environmental change (Khoury et al.,2014; Hunter et al.,2016). For instance, should an insect that damages wheat dramatically increase in abundance during a particular growing season, a region that is focused solely on mass production of wheat will have its entire product decimated. On the contrary, a region that is producing greater crop diversity, might still, on the whole, be successful that season. The amount of processing a particular crop requires has been especially highlighted by the pandemic. During COVID19, meat producers got hit especially hard as workers became infected with the virus and were unable to work. Slow production increased prices and slowed supply of meats across the country. In contrast produce that is processed in more automated ways using machinery (e.g., nuts) was less affected by the Pandemic.
Food Distribution: Much of America’s produce is transported over long distances from farms to urban centers. This transport consumes 10 % of the total energy budget in the U.S. (Gunders, 2012) and contributes to food waste as it spoils or is contaminated enroute (Sachs, 2015). The average meal in the U.S. has traveled 1500 miles from farm to table (CUESA). By the time produce has traveled 1000 miles or more to its destination, it has likely lost substantial nutritional value (Rickman et al.,2007). Reliance on these long food distribution routes threatens food security in urban areas, where over 54% of the World’s population is concentrated (UN, 2018); Reliance on food supply from distant regions puts sustenance of Urban centers at the mercy of natural disasters in distant locations. For instance, when people of the intermountain West rely heavily on produce from California’s Central Valley, their food supply may suffer in the event of large wildfires in California. Furthermore, urban reliance on food produced in distant locations limits accessibility to produce that has short shelf-lives and, therefore, poor transportability. This in turn, increases urban dependence on heavily processed and packaged foods that travel well but do not contain well-rounded nutrition. Many urban areas are turning into “food deserts” in which people do not have ready access to a complete compliment of required nutrients (Walker et al.,2010). Many pre-packaged foods contain excessive amounts of calories, but lack the well-rounded nutrition (i.e., sufficient amounts of vitamins and minerals) that humans need. As a result, urban areas experience a dichotomous problem of nutritional excess, yet insufficiency. This is exemplified by one-third of the world’s people being overweight and/or undernourished (Sachs, 2015; Garnett, 2013; Remans et al.,2014). This problem impacts countries of every economic status (Garnett, 2013). It is now estimated that 19 million Americans now live in food deserts and the Pandemic could double the number of people across the globe that are experiencing food insecurity (Silva, NPR, 27 Sep 2020). Food insecurity may have hit as many as 23% of American households in early 2020, up from 10.5% (13.7 million households) last year (Silva, NPR, 27 Sep 2020). These numbers include people who were not able to obtain enough food to meet their needs or had uncertainty in how to obtain their next meal (Silva, NPR, 27 Sep 2020).During the COVID19 pandemic in early 2020, issues surrounding distribution were observed in the dairy industry. For instance, dairy producers that package and sell to restaurants and schools could no longer do so as restaurants and schools closed during the pandemic. Because of the specificity of their production and distribution lines to restaurants and schools, dairy companies were not able to quickly pivot and redirect milk to other end users. This resulted in a lot of dairy products in both the US and the UK being dumped.
Food Waste Management: 40% of the food produced is never consumed, comprises the largest component of municipal waste and is responsible for a large fraction of annual methane emissions in the United States (Gunders, 2012). Food waste occurs at several different points during its life cycle: 1) food spoil and are thrown away during transport from farms to urban centers, 2) Food spoils or expires on store shelves or in consumer’s homes before it can be eaten, 3) food is wasted during meal preparation in the home (i.e., broccoli stems are trimmed and thrown away instead of eaten), 4) people don’t eat 100% of each meal that they prep and the unwanted food is thrown into the trash. Uneaten food contains vitamins and minerals, that, if composted and returned to the soil, could be used to fuel the production of more nutritious food. But instead, food that is thrown into the trash makes its way to the landfill where nutrition is lost forever rather than being used to recondition our soils and thus allowing us to continue producing food with high nutritional value. In throwing food into the landfill, we are defeating the natural process of composting that replenishes soils of their nutrients. This in combination with farming processes increase erosion and result in nutrients being leached out of soils and washed into rivers and waterways has greatly diminished the quality of our soil and our ability to produce nutritious food. Food waste increased during the COVID19 pandemic as producers were unable to redirect their product to alternative consumers. Potato farmers in Idaho were left with piles of potatoes in the fields that went to waste because restaurants were closed. Some of these potatoes were redistributed to the average consumer and some were trucked off to New York (what did we say above about the problems of long transport lines?), but more waste than usual was incurred. Even cabbage farmers in India, who rub elbows with starving neighbors had excess food waste secondary to people losing their jobs and being unable to buy the produce. But the COVID19 food crisis was not limited to third world countries—it hit hard in the United States too, with many people needing assistance from food banks as jobs dried up and people became unable to afford basic needs (Martin, NPR, Sep 27, 2020). It is estimated that nearly 1 in 4 households in America have experienced food insecurity this year (Silva, NPR, Sep 27, 2020).
Our food System Creates Mineral Deficient Foods
To specifically illustrate how our food system fails in producing food with maximal nutritional value—even in the absence of a Pandemic– we can talk about minerals (i.e., iron, zinc). Because our food system generates foods that are deficient in minerals, over 60%, 30% and 15% of the World’s seven billion people are iron, zinc and selenium deficient, respectively (White and Broadley, 2009). Rates of mineral malnutrition are especially high in Asia and Africa (Muthayya, et al.,2013), where soil degradation is especially severe and has significantly decreased the nutritional value of crops (Lal, 2009). Iron, zinc and selenium are just three of the minerals that the human body needs for overall health and wellness—there are many more, but are beyond the scope of this article. Using iron, zinc and selenium as examples, here are some of the profound effects that they can have on our health in general and can specifically affect one’s course through physical therapy/rehabilitation:
Iron is critical for proper nerve functioning, temperature regulation, immune system function—just to name a few important things. It is also critical for the ability to brain derived neurotrophic growth factor to signal other neurons and assist one’s body with learning new motor patterns—a concept known as neuroplasticity. After neurological injury (i.e., stroke) or in the presence of a degenerative neurological condition (i.e., Parkinson’s Disease) it is especially important that good nutrition be part of a physical rehabilitation program so that the body can optimally learn and perform new movement skills.
Zinc plays important roles in motor function (again, especially important for physical rehabilitation!), immune system function, mood and improving attention span (both of which are critical for learning!).
Selenium is very important for cognitive function, immune system support and thyroid metabolism. Thyroid metabolism is critical in maintaining one’s energy and mood and motivation for effortful things such as physical rehabilitation.
More than likely, you or someone you know are affected by one or more of these deficiencies. And with improved nutrition, their overall quality of life and ability to maximize their potential could be greatly enhanced.
WORKING TOWARDS SOLUTIONS
The solution lies in getting to the root of the problem—literally. To summarize in the simplest way possible: 1) The problem begins with our soils, which are being more and more nutrient depleted through the years and crop plants do not have access to enough nutrients to produce a nutritious end product. 2) We then transport food long distances from farm to table, during which it loses more nutrition. 3) We then throw away a lot of food either as it spoils enroute to supermarkets, during prep or after it spoils in individual households; the food that goes to the landfill rots and produces greenhouse gases rather than being composted by mother nature to replenish the soil for growing the next crop. This means that we need a three-part solution which includes the following 1) bringing the farm closer to the table, 2) reducing overall food waste and 3) properly composting unavoidable food waste in order to replenish our soils with the nutrients needed to grow the next nutritious crop.
There are solutions in the works on bigger scales through the regenerative agriculture movement, which is shifting farms away from traditional industrial farming. Regenerative agriculture includes methods that do not apply chemicals and fertilizers at massive scales, involve no till methods to preserve our soils and, overall, work with mother Nature rather than against her. A review of regenerative agriculture is beyond the scope of this article and you can learn more about that here: Dr. Mark Hyman. Can regenerative agriculture really heal humans and the planet?. While regenerative agriculture could greatly improve the quality of the foods that are being produced and prevent degradation of the land, it requires wide adoption across the United States to make it effective in improving public health which will take time and it does not necessarily solve the fact that food would still be traveling 1000’s of miles to market. We need a solution in the interim that people can act on now and have healthy food on their table quickly.
So what is a concerned physical therapist to do? Let’s first talk about the role of a physical therapist in patient nutrition.
A physical therapist’s role in patient nutrition
It’s been slow for the masses—and even those within the physical therapy profession—to realize and embrace that it is within our scope of practice to educate patients on nutrition. In fact, in a seminal paper published back in 2009, physical therapist Elizabeth Dean, stated that “….physical therapists are uniquely qualified to lead in the assault on lifestyle conditions” (Dean 2009). She also goes on to note that in leading the assault on lifestyle conditions, physical therapists are positioned to promote the health of communities. The American Physical Therapy Association’s stance on the role of physical therapists in patient nutrition is that “it is within the professional scope of physical therapist practice to screen for and provide information on diet and nutritional issues to patients, clients, and the community.” (APTA). While physical therapists certainly don’t replace registered dieticians who can come up with very specific nutritional plans, physical therapists can be instrumental in screening for nutritional red flags and educate patients on what avenues might be good to go down with their nutrition as well as what specifics may be important to pay attention to given a patient’s unique situation. For example, those with rheumatoid arthritis may want to consider a Mediterranean Diet which has been shown to reduce overall levels of inflammation in the body (Arthritis Foundation).
However, a physical therapist’s job becomes more difficult when the problem has deeper roots than someone simply not eating the right foods. Even when all of us eat the “right foods” we are likely not getting a full complement of vitamins and minerals due to our failing food system.
So can a physical therapist still play a role in solving this problem? If we take an unconventional approach, I believe the answer is yes. We need to add some elements to our education—which include empowering people to produce some of their own food. And YES. The great majority of people living in all kinds of climates and parts of the country CAN do this.
What I am doing to change the face of nutritional education
As a former professor and researcher at Idaho State University (Pocatello, ID, USA), I began developing a method for sustainable agriculture that can be implemented in even the smallest of urban apartments. My students and I determined that by composting household wastes (i.e., vegetable scraps, paper, coffee filters), we could reduce the waste of a single person household by 46% all while generating compost that we could utilize to grow nutrient rich greens—microgreens specifically. To do this, we used a commercially available vermicomposter from Uncle Jim’s Worm Farm (https://unclejimswormfarm.com). Yes—vermicomposting means composting with worms.
In doing so, individuals could reduce their dependence on buying produce from the supermarket that had traveled 1000’s of miles from the farm where it was produced using methods that are resource heavy and degrade soils. All the while, individuals could increase their food security and nutritional intake by bringing their farm and table right next to each other.
For those of you who haven’t heard of microgreens, they are the edible seedlings that are usually harvested seven to fourteen days after germination when they have two fully developed cotyledon leaves (Xiao et al. 2012). A wide variety of herbs (e.g., basil, cilantro), vegetables (e.g., radish, broccoli, mesclun) and even flowers (e.g., sunflowers) are grown as microgreens. Microgreens are generally more flavorful, some of them quite spicy, than their mature counterparts and have grown in popularity among culinary artists for adding texture and flavor accents to salads, sandwiches and other dishes (Treadwell et al. 2010; Wallin, 2013). The increasing culinary demand as well as the ease with which microgreens can be grown, even by inexperienced gardeners in urban settings, has piqued interests in growing and eating them. Interest in microgreens has also been generated by popular websites (e.g., Warner, 2012) touting the findings of Xiao et al.(2012), which indicate that microgreens may have four to 40 times the amount of some nutrients and vitamins as the vegetables a mature plant would produce. However, Xiao et al.(2012) note that the nutritional aspects they measured varied widely among microgreen types, providing fodder for future study and Weber (2016) noted that the methods used to grow microgreens (i.e., soil, compost, hydroponic) can significantly impact their nutritional value. Additionally, a systematic comparison of the environmental impacts (i.e., water use, nutrient demand) of microgreen cultivation methods has not been conducted and should be considered alongside their impacts on nutritional value when deciding how to grow microgreens and if they provide a nutrient-rich crop that can be sustainably produced.
You can also use these methods to produce baby greens which are a more mature stage of growth than the microgreen stage.
If each one of us could begin producing even some of our own produce using sustainable methods for composting household waste, we could greatly reduce out impact on the environment, increase our food security, relying less on produce that is transported 1000’s of miles and increase our nutritional intake. I call this distributed Agriculture—each household operating as its own little producer. Distributed agriculture makes one more resilient to environmental and socioeconomic change that is going on in the world outside of our homes. We specifically looked how growing and consuming broccoli microgreens could reduce impact on the environment relative to consuming broccoli vegetable that is produced in California’s Central Valley. To summarize quickly, broccoli microgreens can go from seed to harvest in 7 days (93-95% less time than needed to produce broccoli vegetable), there is no need for fertilizer, distance of transport from farm to table is zero, and the mineral nutrition the microgreens is 1.73 times that of the vegetable with respect to iron, zinc, magnesium and calcium among other minerals (Weber, 2017). The full summary of this data was published in Frontiers in Nutrition in 2017 (Weber, 2017).
In addition to the above benefits, growing one’s own food has been shown to be great for reducing stress and enhancing a sense of pride in being able to be more self-sufficient. The therapeutic effects of growing one’s own food have been proven in many studies and in case you didn’t know there is a form of therapy called Horticultural Therapy. The therapeutic effects span across all ages and include improved concentration, memory, cognitive function, fine motor skills, personal satisfaction as well as decreased heart rate, stress, and anxiety (Haller et al. 2019).
If you are interested in learning more about the methods for taking charge of your nutrition and growing your own produce at home, please contact me. I am currently producing an online course and you can be the first to know when it is being released! I have had the pleasure of teaching/Lecturing about this topic within the past few years at County Extension Offices in Iowa and the Greater Des Moines Botanical Garden (Des Moines, IA, USA). Due to the pandemic and the widespread need of this information, I am hoping that a digital course will make this more accessible to the masses.
REFERENCES CITED AND RESOURCES FOR MORE INFORMATION
Dean, E. 2009. Physical therapy in the 21st Century (Part I): Toward practice informed by epidemiology and the crisis of lifestyle conditions. Physiotherapy Theroy and Practice, 25(5): 330-353.
Garnett, 2013 Symposium I: sustainability and food security, food sustainability: problems, perspectives and solutions. Proc Nutr Soc (2013) 72:29–39.
Gunders, 2012. Wasted: How America Is Losing up to 40 Percent of Its Food from Farm to Fork to Landfill. National Resources Defense Council Issue Paper. IP: 12-06-B. Available from: < https://www.nrdc.org/sites/default/files/wasted-food-IP.pdf > accessed: 29 Nov 2020.
Haller et al. 2019. The profession and practice of horticultural therapy. CRC Press. Taylor and Francis, Boca Raton, FL.
Hunter et al. 2016. Enabled or disabled: is the environment right for usingbiodiversity to improve nutrition? Frontiers in Nutrition. 3:14. doi:10.3389/fnut.2016.00014
Khoury et al. 2014 Increasing homogeneity in global food supplies and the implications for food security. Proc Natl Acad Sci U S A. 111(11):4001–6.
Lal R. 2009. Soil degradation as a reason for inadequate human nutrition. Food Secur. 1:45–57. doi:10.1007/s12571-009-0009-z
Muthayya et al. 2013. The global hidden hunger indices and maps: an advocacy tool for action. PLoS One. 8(6):e67860. doin:10.1371/journal.pone.0067860.
Remans et al. 2014. Measuring nutritional diversity of national food supplies. Global Food Secur. 3:174–82. doi:10.1016/j.gfs.2014.07.001
Rickman et al. 2007. Nutritional comparison of fresh, frozen and canned fruits and vegetables. Part 1. Vitamins C and B and phenolic compounds. J Sci Food Agric. 87:930–44.
Sachs, 2015. Chapter 10 food security. The Age of Sustainable Development. New York: Columbia University Press. p. 317–53.
Sliva. C. 27 Sep 2020. NPR. Food Insecurity in the US by the Numbers. https://www.npr.org/912486921 accessed: 29 Nov 2020.
Treadwell D, Hochmuth R, Landrum L, Laughlin W. 2010. Microgreens: A New Specialty Crop. Gainesville, FL: University of Florida IFAS Extension HS1164.
Walker et al. 2010. Disparities and access to healthy food in the United States: a review of food deserts literature. Health Place. 16(5):876–84. doi:10.1016/j.healthplace.2010.04.013
Wallin C. 2013. Growing Microgreens for Profit. Anacortes, WA: Headstart Publishing, LLC.
Weber CF. Nutrient concentration of cabbage and lettuce microgreensgrown on vermicompost and hydroponic growing pads. J Hortic (2016) 3:4. doi:10.4172/2376-0354.1000190
White and Broadley, 2009. Biofortifying crops with essential mineral elements. Trends Plant Sci (2005) 10(12):586–93. doi:10.1016/j.tplants.2005.10.001
Xiao et al. 2012. Assessment of vitamin and carotenoid concentrations of emerging food products: edible microgreens. J Ag. Food Chem. 60: 7644-7651.
Patients with Parkinson’s Disease (PD) often develop respiratory weakness and lower lung capacities. This greatly diminishes quality of life, leading to difficulties with breathing, speaking, and swallowing. Respiratory weakness can also lead to one of the most common causes of death in people with Parkinson’s Disease –aspiration pneumonia—especially in the late stages of the disease.
Individuals with PD can experience over 50% decreases in maximum inspiratory pressure and maximum expiratory pressure, which is essentially the force with which one can inhale or exhale, respectively (Sapienza et al. 2011). Poor ability to inhale may be attributable to reduced respiratory muscle strength and increased chest wall rigidity (Sathyaprabha et al. 2005), which are two common characteristics of PD.
In short, living the best possible life with PD includes taking preventative measures to reduce PD’s impact on the respiratory system. There are currently no standard protocols for respiratory therapy for people with PD, but research is beginning to show some promise for exercising the respiratory system –just like one should exercise the rest of the body.
Respiratory Muscle Training (RMT)
Research on techniques to improve respiratory health is in its infancy, but some studies have indicated that a technique called Respiratory Muscle Training (RMT) may significantly improve respiratory muscle strength (Jones and Busse, 2012). RMT involves inhaling and/or exhaling against resistance through a device called a respiratory muscle trainer.
Proper posture for respiratory muscle training (source: Sapienza et al. 2011)
Research has shown that RMT can increase respiratory muscle strength (Sapienza et al. 2011 Reychler et al. 2016). Put simply, RMT can improves one’s ability to cough, breathe, swallow and talk at normal volume. This leads to the following improvements in quality of life:
A good strong cough = clearing secretions and foreign objects from the airways
Ease with swallowing=prevention of choking, aspiration (getting food into the airways) and subsequent infection and pneumonia that could develop.
Talking with adequate volume= improved communication and social relationships.
Two forms of RMT have been examined: inspiratory muscle strength training (strength for inhaling) and expiratory muscle strength training (strength for exhaling).
In a study of 60 participants, half of which were randomly chosen to utilize a expiratory muscle strength trainer (EMST) for 4 weeks while the other group utilized a sham device, EMST was found to increase maximum expiratory pressure by 27%, improve swallowing function (Sapienza et al. 2011). Other studies have also demonstrated that EMST can improve coughing and a reduction in incidence of aspiration (Troche et al. 2010; Pitts et al. 2009). In short, EMST can make critical improvements in strength that protect lungs from aspiration and subsequent pulmonary complications.
Studies of inspiratory muscle strength training in people with PD are currently underway (Ferro et al. 2019). However, a study that has been done on healthy adults over the age of 65 does demonstrates that (IMST) may have serious benefits in improving maximum inspiratory pressure (Reychler et al. 2016). Over the course of a 4-week IMST program, 16 participants were able to increase their maximum inspiratory pressure by 38% (Reychler et al. 2016). Over the course of the 4 weeks, participants performed 15 minutes of IMST maintaining a respiratory rate of 15-20 breaths per minute; each week of the program, the resistance on their training device was increased (Reychler et al. 2016).
A device on the market that allows one to perform RMT for inspiratory and expiratory muscles is THE BREATHER (click on image below to see in store and purchase):
To see a product demo video of THE BREATHER, click here.
Using such a device, improvements in respiratory muscle strength can seen in as little as 4 weeks, but it must be utilized at high frequency daily. For instance, in the Sapienza et al. (2011) study, participants performed 5 sets of 5 repetitions of EMST exercise, on 5 days per week. Although it takes dedication, improvement in respiratory muscle strength can be seen in a little as 4 weeks according to Sapienza et al. (2011). Similarly, healthy geriatric patients had improved inspiratory muscle strength over the course of 4-weeks when practicing IMST for 15 minutes on 5 days per week (Reychler et al. 2016).
Can other people besides those with Parkinson’s Disease benefit from RMT?
In addition to benefitting those with Parkinson’s Disease, RMT can improve quality of life for those with other neurodegenerative conditions (i.e., ALS (Lou Gherig’s Disease), multiple sclerosis, Huntington’s Disease; Jones and Busse, 2012)—-and even athletes and musicians without neurodegenerative conditions.
Weber Physical Therapy and Wellness can get you started on an RMT program. As an RMT patient, you can expect the following:
initial evaluation at which you will be trained in and provided with a home exercise program.
one visit with your therapist per week for 4-6 weeks to check in with your progress and to adjust your home exercise program.
Transition to self-guided home exercise program to continue on your own for maintenance and follow up with therapist only if needed.
If you have questions about this program and whether it may be right for you, please get in touch with Carolyn Weber via phone (505-412-8384) or email (cfweberpt@gmail.com).
References:
Ferro et al. 2019. Effects of inspiratory muscle training on respiratory muscle strength, lung function, functional capacity and cardiac autonomic function in Parkinson’s disease: randomized controlled clinical trial protocol. Physiotherapy Research Int. 24(3). Doi: 10.1002/pri.1777.
Jones and Busse. 2012. Management of respiratory problems in people with neurodegenerative conditions: a narrative review. Physiotherapy. 98:1-12.
Pitts et al. 2009. Impact of expiratory muscle strength training on voluntary cough and swallow function in Parkinson disease. Chest. 135(5): 1301-1308.
Reychler et al. 2016. Randomized controlled trial of the effect of inspiratory muscle training and incentive spirometry on respiratory muscle strength, chest wall expansion and lung function in elderly adults. Journal of the American Geriatrics Society. Http://doi.org/10.1111/jgs.14097
Ribeiro et al. 2018. Breath stacking and incentive spirometry in Parkinson’s Disease: randomized crossover clinical trial. Respiratory Physiology and Neurobiology. 255: 11-16.
Sapienza et al. 2011. Respiratory strength training: concept and intervention outcomes. Seminars in speech and language. 32(11): 21-30.
Sathyaprabha et al. 2005. Pulmonary functions in Parkinson’s Disease. Indian Journal of Chest Disease Allied Sci. 47(4): 251-257.
Troche et al. 2010. Aspiration and swallowing in Parkinson’s Disease and rehabilitation with EMST: the ASPIRE study. Neurology. 75(21): 1912-1919.
It’s summer in Southeast, Idaho and the road-biking couldn’t be any better. Long country roads in the mountains to challenge the legs and sweet-smelling air to fill the lungs.
Early Summer in Southeast, Idaho
But wherever you are, I am sure that you want to enjoy road cycling too. Now and well into the future. Key to this, is staying injury and pain free. While cycling is associated with being low-impact and lower injury risk than other sports, there are still some issues that can crop up that would be best avoided to keep the joy in joy-riding. Below are 11 tips regarding bike fit and biomechanics that are important in avoiding pain and injury.
Saddle: Be sure that your saddle is level. If you are sliding too far forward, you will have too much weight being placed on your hands, arms and lower back. If the seat is tilted backwards, you may place strain on your lower back and experience pain in your own saddle area. The saddle should be a comfortable distance from the handlebars–if it is too close to the handlebars, more weight will be placed on the arms and mid back; if the saddle is too far from the handlebars, there will be more strain on the low back and neck. Saddle height should be placed by someone who can help you assess your knee angle when you are sitting in the seat. When your leg is in its most extended position (the point in peddling when your foot is at its lowest point going around the cranks) your ideal knee angle should be close to 35 degrees (see picture below) to lessen stress on the knee. Recommended knee angles for recreation cyclists are 35-45 degrees and for road cyclists are 30-35 degrees. Your knee should be slightly bent at the bottom of the pedal stroke.
Diagram from American Physical Therapy Association.
Diagram from American Physical Therapy Association.
2. Handlebars: The higher the handlebars, the more weight will be placed on the saddle. Taller riders should have lower handlebars in relation to the height of the saddle. Proper handlebar position allows for the shoulder to make a (roughly) 90 degree angle between the upper arm and trunk. Trunk angle for the road cyclist is 25-35 degrees and for comfort/recreational riding is 35-90 degrees.
3. Foot position on the pedal: The ball of the foot should be positioned over the pedal spindle for the best leverage, comfort and efficiency. A stiff-soled show is the best for comfort and performance.
4. Hand position: Change your hand position on the handlebars frequently for upper body comfort and prevent nerve compression in the hands and wrists. Use a controlled and relaxed grip. If you are experiencing numbness in your wrists or hands the above could be a problem–or you may have bike fit problems discussed above that put too much pressure through the arms and hands (e.g., short reach handlebars, handlebars placed too low, saddle tilted forward, saddle too far forward).
5. Cadence: Or sometimes known as revolutions per minute. Each foot should be going around the cranks at a rate of 80-90 revolutions per minute (advanced cyclists 90-105 revolutions per minute)–without bouncing up and down in the seat. Maintaining a high cadence places less stress on the lower back and knees.
6. Don’t rock your hips back and forth: Your should be using your core strength to stabilize your hips so that they are not rocking back and forth. You may notice yourself falling into this when fatigued. If you are doing this right out of the gate, you may have a bad bike fit. Rocking back and forth causes friction between you and the seat and can just get plain uncomfortable.
7. Anterior (front) knee pain: Possible causes of this include pedaling at too low of a cadence (see “5” above), overusing your quadriceps muscles, misaligned bike cleat (see “3” above) and muscle imbalance in your legs (strong quads and weak hamstrings).
8. Lower back pain: you may have tight hamstrings, low cadence overuse of quads, poor back strength and too long or too low handlebars.
9. Foot numbness or pain: you may be overusing the quads, have low cadence that places a lot of pressure through the feet or a maligned bike cleat.
10. neck pain: you may have too low of handlebars, handlebars that tare too far away or too close or your saddle may have a downward tilt.
11. liliotibial band pain (ITB): your saddle may be too high, bike cleats are maligned or you may have a leg length discrepancy.
If you feel as though you need some help with bike fit or that your pain is stemming from injury, despite a proper bike fit, your physical therapist is here to help. You do NOT need a referral from your doctor–or even use your insurance–to see me. Contact me to see if working with me on your bike issues is right for you—talking is always free.
2017 USA Triathlon National Championships in Omaha, Nebraska
Physical pain is common. Everyone will experience it at some point in his or her life. Often, pain will result from an injury and will resolve when the injury heals. This is normal. This is good news for the 84% of us who will likely experience something like low back pain in our lives. It will come and go and we will go on our marry way. But for many, this pain lingers and has become the most common cause of disability and time off work in people over the age of 45 (Balagué et al. 2012). Long term, or chronic pain, that results in disability is a much bigger issue. What’s worse is that many of these people end up relying on opioid drugs (prescription and not) in attempts to manage their pain.
Opioids and the crisis
Opioid use has sky-rocketed in recent years, and drug overdose deaths are on the rise. So much so that the Center for Disease Control (CDC) has declared that we are in the middle of an “opioid crisis” and it is an epidemic. This epidemic is not just affecting the heroin addict living in the back alley. It’s everyday people who rely on opioids to cope with pain (i.e., low back pain, knee pain). The statistics are staggering:
From 1999 to 2017, more than 700,000 people have died from drug overdose.
Around 68% of the more than 70,200 drug overdose deaths in 2017 involved an opioid.
In 2017, the number of overdose deaths involving opioids (including prescription opioids and illegal opioids like heroin and illicitly manufactured fentanyl) was 6 times higher than in 1999.
Despite this, it is important to note that THERE IS a time and place for taking opioids—for instance, following significant surgery or injury when managing pain is difficult without them. However, prolonged use of opioids long after recovery from surgery or traumatic injury can result in addiction and can cause people to rely on opioids long term. The reason that people become addicted to opioids is that they only mask the sensation of pain—they do not alter the source of the pain. This is not to mention that the withdrawal symptoms are severe. It’s hard to get off of opioids. This is the vicious cycle of addiction. Taking opioids long term also has side effects of depression, for which many people take more drugs. This is why there are important Questions to ask your doctor about pain medication when they are writing you a prescription. Even the most well-meaning doctors can send you down the road of addiction without meaning to.
Long story short, opioids are a “bandaid” for pain and getting to the root of the problem requires understanding why someone enters a state of chronic pain. If an injury is healed and there is no more tissue damage or new injury, then why can one still hurt? This is what is important to get a handle on. Many factors play a role in creating each person’s unique “pain experience” which includes emotions, thoughts and beliefs—it’s not just physical. Read on…
Understanding Pain
Research has shown that when people understand pain, they can better manage their pain. And when one can manage his or her own pain, he or she can take life by the horns again. Simply put:
“Know pain, know gain”—David Butler
This is especially true for people dealing with chronic pain. Many people have an overly simplistic view of how pain is experienced. And I say “experienced” very deliberately. As children, we learn that doing something such as touching a hot stove or stepping on a sharp object with bare feet creates pain. These two events are generally associated with tissue damage—the skin is compromised and you get a blister or a stab wound. But the shocking thing to most people is that this pain does not originate in the injured part of the body. Pain is an experience that is created in the brain once it interprets the signals that the rest of the body send to it. So when you step on a nail, the sensory cells send signals all the way up the spinal cord to your brain where you brain interprets this event as being painful. Obviously, this occurs in fractions of second and you generally pull your foot away from the nail. In this experience, the interpretation of pain is a good thing—it signifies that there is a threat in your environment (the nail) that you harm you.
The fact that pain is an experience that is created by the brain explains why two soccer players can experience the same injury on the field and one gets up and keeps playing while the other lays on the ground crying out for help. It also explains why people can experience pain in a body part without actual threat to it. Say you had a traumatic experience as a child when you stepped on a rusty nail with bare feet and you ended up in the hospital with pain and a raging infection in your foot. Now, when you so much as look at a rusty nail you experience pain in your foot. You foot is healed and the nail is no where near your foot. Danger is absent, injury is absent……but pain is ever present. This experience is created purely in the brain.
Below are a few videos from some of the World’s leading pain experts. Watch them to learn more about how your pain experience is created ….. and how you can take control.
Below, Professor Lorimer Mosely explains how pain works. Pain evolved as a protective mechanism to indicate when the body was in danger. However, when our experiences change the way that pain is experienced and skews what the pain is indicating, it can result in a maladaptive response—or extreme fear from harmless sensation (i.e., a tree branch brushing one’s leg on a hike).
Each part of your body is represented on a specific area of the brain. There is a part of your brain dedicated to being able to detect sensation of your left pinky finger—and every other part of your body. If you experience prolonged pain in your left pinky finger, the “sharpness” of left pinky’s representation on the brain is lost and you brain can no longer create a pain experience in just your left pinky. Maybe then your neighboring fingers begin to hurt and the pain becomes more widespread. This is phenomena is known as brian smudging as explained below by expert David Butler.
If you have recurring or ruminating thoughts of your pain, that is a sure recipe for making your pain worse. Yes—pain has a significant emotional component. These recurring thoughts have been termed “thought viruses”.
Myth: getting high tech imaging of your painful area will explain the source of your pain.
Professor Peter O’Sullivan explains the discrepancy between medical imaging and pain and how thoughts, and beliefs and movement habits actually matter more.
It’s only 1% of back pain that is really serious stuff….99% has no diagnosis based on scan”. Peter O’Sullivan.
Physical Therapy is a safe alternative to opioids for pain management
If you watched the video above with Professor Peter O’Sullivan, you will have learned that many people with low back pain get medical imaging (i.e., MRI, X-rays, CT scans) that lead them to believe that their backs were really “messed up” structurally. As a result, they developed fear of further injury and starting moving (or not moving) in ways that actually exacerbated their pain—-it wasn’t the “bulging disc” that might have been found on imaging.
“Pain does not equal structural injury” –Prof. Peter O’Sullivan
Restoring healthy movement patterns in conjunction with understanding pain is essential to managing back pain. Physical therapists can help you do both. Even better, physical therapy can not only get you moving better again, they can get you back to an more active lifestyle that includes activities that you love doing. This is why the CDC has recommended physical therapy as a safe alternative to opioids for pain management.
Resources for helping managing chronic pain have been compiled by the ChoosePT movement organized by the American Physical Therapy Association (APTA).
If you would like to delve deeper into these topics, here are two books that I would highly recommend. Click on the images to see details.
Weber Physical Therapy and Wellness supports the ChoosePT movement. If you are experiencing chronic pain and would like a free consult to see how physical therapy can help you, please get in touch or schedule a free consultation: Schedule Appointment
***
References and helpful websites:
Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. The Lancet. 2012;4(379): 482-91.
Rundell SD, Davenport TE. Patient education based on principles of cognitive behavioral therapy for a patient with persistent low back pain: a case report. J Orthop Sports Phys Ther. 2010:40:494–501.
Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis [erratum in: N Engl J Med. 2013;369:683]. N Engl J Med. 2013;368:1675-1684.
Longo UG, Franceschi F, Berton A, et al. Conservative treatment and rotator cuff tear progression. Med Sport Sci. 2012;57:90–99.