It’s summer in Southeast, Idaho and the road-biking couldn’t be any better. Long country roads in the mountains to challenge the legs and sweet-smelling air to fill the lungs.

Early Summer in Southeast, Idaho
But wherever you are, I am sure that you want to enjoy road cycling too. Now and well into the future. Key to this, is staying injury and pain free. While cycling is associated with being low-impact and lower injury risk than other sports, there are still some issues that can crop up that would be best avoided to keep the joy in joy-riding. Below are 11 tips regarding bike fit and biomechanics that are important in avoiding pain and injury.
- Saddle: Be sure that your saddle is level. If you are sliding too far forward, you will have too much weight being placed on your hands, arms and lower back. If the seat is tilted backwards, you may place strain on your lower back and experience pain in your own saddle area. The saddle should be a comfortable distance from the handlebars–if it is too close to the handlebars, more weight will be placed on the arms and mid back; if the saddle is too far from the handlebars, there will be more strain on the low back and neck. Saddle height should be placed by someone who can help you assess your knee angle when you are sitting in the seat. When your leg is in its most extended position (the point in peddling when your foot is at its lowest point going around the cranks) your ideal knee angle should be close to 35 degrees (see picture below) to lessen stress on the knee. Recommended knee angles for recreation cyclists are 35-45 degrees and for road cyclists are 30-35 degrees. Your knee should be slightly bent at the bottom of the pedal stroke.

Diagram from American Physical Therapy Association.

Diagram from American Physical Therapy Association.
2. Handlebars: The higher the handlebars, the more weight will be placed on the saddle. Taller riders should have lower handlebars in relation to the height of the saddle. Proper handlebar position allows for the shoulder to make a (roughly) 90 degree angle between the upper arm and trunk. Trunk angle for the road cyclist is 25-35 degrees and for comfort/recreational riding is 35-90 degrees.
3. Foot position on the pedal: The ball of the foot should be positioned over the pedal spindle for the best leverage, comfort and efficiency. A stiff-soled show is the best for comfort and performance.
4. Hand position: Change your hand position on the handlebars frequently for upper body comfort and prevent nerve compression in the hands and wrists. Use a controlled and relaxed grip. If you are experiencing numbness in your wrists or hands the above could be a problem–or you may have bike fit problems discussed above that put too much pressure through the arms and hands (e.g., short reach handlebars, handlebars placed too low, saddle tilted forward, saddle too far forward).
5. Cadence: Or sometimes known as revolutions per minute. Each foot should be going around the cranks at a rate of 80-90 revolutions per minute (advanced cyclists 90-105 revolutions per minute)–without bouncing up and down in the seat. Maintaining a high cadence places less stress on the lower back and knees.
6. Don’t rock your hips back and forth: Your should be using your core strength to stabilize your hips so that they are not rocking back and forth. You may notice yourself falling into this when fatigued. If you are doing this right out of the gate, you may have a bad bike fit. Rocking back and forth causes friction between you and the seat and can just get plain uncomfortable.
7. Anterior (front) knee pain: Possible causes of this include pedaling at too low of a cadence (see “5” above), overusing your quadriceps muscles, misaligned bike cleat (see “3” above) and muscle imbalance in your legs (strong quads and weak hamstrings).
8. Lower back pain: you may have tight hamstrings, low cadence overuse of quads, poor back strength and too long or too low handlebars.
9. Foot numbness or pain: you may be overusing the quads, have low cadence that places a lot of pressure through the feet or a maligned bike cleat.
10. neck pain: you may have too low of handlebars, handlebars that tare too far away or too close or your saddle may have a downward tilt.
11. liliotibial band pain (ITB): your saddle may be too high, bike cleats are maligned or you may have a leg length discrepancy.
If you feel as though you need some help with bike fit or that your pain is stemming from injury, despite a proper bike fit, your physical therapist is here to help. You do NOT need a referral from your doctor–or even use your insurance–to see me. Contact me to see if working with me on your bike issues is right for you—talking is always free.

2017 USA Triathlon National Championships in Omaha, Nebraska





 Running is stressful on the body and so is child-birth. Doing these two things too closely back to back can have adverse consequences. This is evidenced by the prevalence of urinary incontinence, pelvic organ prolapse (POP), abdominal muscle separation and pain that are experienced by female runners after having a baby. Urinary incontinence and POP can result from the stress that is place on the pelvic floor muscles. For a review of the anatomy of the pelvic floor muscles click
Running is stressful on the body and so is child-birth. Doing these two things too closely back to back can have adverse consequences. This is evidenced by the prevalence of urinary incontinence, pelvic organ prolapse (POP), abdominal muscle separation and pain that are experienced by female runners after having a baby. Urinary incontinence and POP can result from the stress that is place on the pelvic floor muscles. For a review of the anatomy of the pelvic floor muscles click 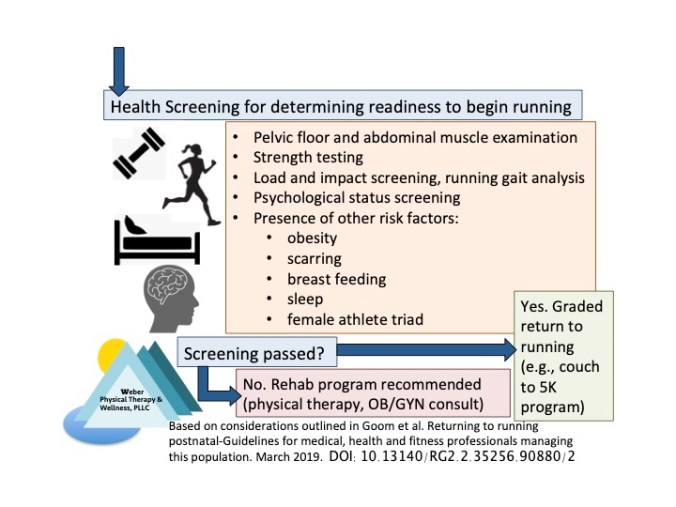 The screening process is recommended to cover the following:
The screening process is recommended to cover the following: