You’ve had your baby. Other than the sleepless nights, you’re absolutely smitten. But just when it seems that you couldn’t possibly have any more love to divvy out, you’d really like to give some love to your running shoes and favorite trails.
But are you physically and mentally ready for running?
This is the million-dollar question.
Truth be told, medical guidelines for determining readiness for you to return to running are in their infancy—pun intended. Relatively speaking, there have not been a lot of extensive research studies to determine hard and fast guidelines for medical practioners to help guide you through this exciting and challenging transition in your life. However, physical therapists Tom Goom, Grainne Donnelly and Emma Brockwell, have compiled the evidence that does exist as well as their extensive clinical experience to help safely guide women back to running. What they have published is a beautiful foundation for providing advice to women at present and for building on as new research in post partum running reveals new information. I will summarize some key points from this publication below.
“Return to running is not advisable prior to 3 months postnatal or beyond this if any symptoms of pelvic floor dysfunction are identified prior to, or after attempting, return to running” (Goom et al. 2019).
 Running is stressful on the body and so is child-birth. Doing these two things too closely back to back can have adverse consequences. This is evidenced by the prevalence of urinary incontinence, pelvic organ prolapse (POP), abdominal muscle separation and pain that are experienced by female runners after having a baby. Urinary incontinence and POP can result from the stress that is place on the pelvic floor muscles. For a review of the anatomy of the pelvic floor muscles click here. Post vaginal delivery, the levator ani muscles, which are part of the pelvic floor, take 4-6 months to reach maximum recovery. When you consider that the impact of running increases the risk 4.59 times of pelvic floor muscle dysfuntion (vs. low impact sports like cycling), you can start to see why it is recommended to wait at least a few months post child-birth prior to running. If you have had your baby via C-section, additional time for healing is needed. At 6 weeks post C –section, the uterine scarring is still very much healing and abdominal tissue, known as fascia, is only 51-59% as strong as it originally was. Even 6-7 month after a C-section, abdominal fascia is only 73-93% of its original strength.
Running is stressful on the body and so is child-birth. Doing these two things too closely back to back can have adverse consequences. This is evidenced by the prevalence of urinary incontinence, pelvic organ prolapse (POP), abdominal muscle separation and pain that are experienced by female runners after having a baby. Urinary incontinence and POP can result from the stress that is place on the pelvic floor muscles. For a review of the anatomy of the pelvic floor muscles click here. Post vaginal delivery, the levator ani muscles, which are part of the pelvic floor, take 4-6 months to reach maximum recovery. When you consider that the impact of running increases the risk 4.59 times of pelvic floor muscle dysfuntion (vs. low impact sports like cycling), you can start to see why it is recommended to wait at least a few months post child-birth prior to running. If you have had your baby via C-section, additional time for healing is needed. At 6 weeks post C –section, the uterine scarring is still very much healing and abdominal tissue, known as fascia, is only 51-59% as strong as it originally was. Even 6-7 month after a C-section, abdominal fascia is only 73-93% of its original strength.
What are some indicators of pelvic floor or abdominal wall dysfunction?
- Urinary and/or fecal incontinence
- Urgency that is difficult to defer
- Heaviness/pressure/bulging/dragging in the pelvic area
- Obstructive defecation: characterized by feeling that stool remains in your rectum even after trying to pass it, excessive straining, need to use laxative or enemas to pass stool
- separated abdominal muscles and/or decreased abdominal strength and function
- low back or pelvic pain
- Ongoing or increased blood loss beyond 8 weeks post child-birth that is not linked to your menstrual cycle.
If you are experiencing any of these symptoms you are definitely not ready for running and should seek medical care.
If you are 3 months post child-birth and do not have any of the above symptoms, it is recommended that you have a complete health screening and risk assessment done to ensure readiness for graded return to running.
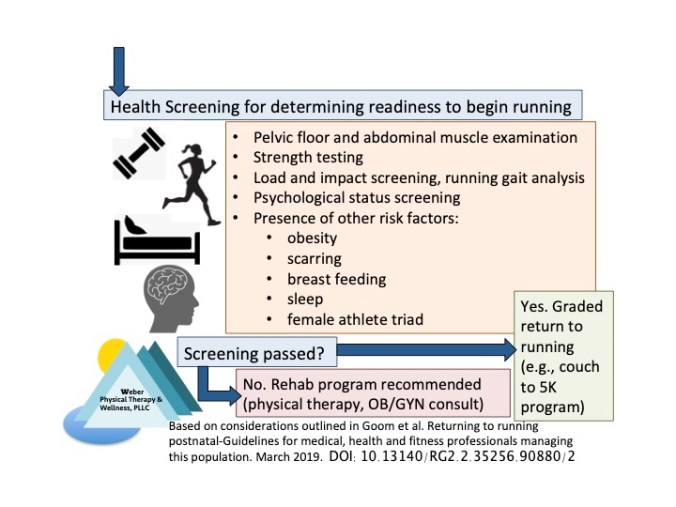 The screening process is recommended to cover the following:
The screening process is recommended to cover the following:
Load and impact management assessment: Your physical therapist can assess you ability to walk, squat, hop, jog with good mechanics and without pain, incontinence or feelings of heaviness in the pelvic floor. Your pelvic floor, abdominal and leg strength should also be assessed.
Gait analysis: It recommended that your running form be reviewed to look for significant injury risk factors. This is something that an experienced physical therapist can provide for you.
Preexisting pelvic or lumbar spine dysfunction or hypermobility conditions (e.g., Ehlers Danlos): If you were having pelvic or low back issues or joint laxity prior to or during pregnancy, you should exercise caution in returning to running and this may exacerbate problems associated with joint laxity.
Fitness level: Generally speaking, women who maintained high levels of fitness before and during pregnancy, usually bounce back faster. If you were fairly sedentary and are now looking to increase your physical fitness post-baby—that’s awesome, but you’ll need to take that into consideration when trying to take up exercise and/or running.
Breathing: Proper breathing, which is important for running, may need to be restored post-baby to recreate proper synergy between pelvic floor, abdominal muscles and diaphragm.
Psychology: Postnatal depression is experienced by 20% of mothers and it needs to be considered in the context of return to running. Obsessive focus on returning to pre-pregnancy fitness and taking running to a level that is too intense for the stage of post partum recovery can result in injury.
Diastasis rectus abdominis: Core strength is important for efficient and injury free running. If you have separated abdominal muscles, you will need to rehab these to minimize injury risk with running.
Scar mobility: Adhesions in C-section scars can create tension, pain and alter the function of muscles in this region, resulting in subpar running mechanics.
Breastfeeding: maintains lower levels of estrogen and continued elevated levels of relaxin, which may or may not contribute to increased laxity of joints. Running should be timed carefully around breast-feeding so that you are not running with your breasts overly full, which can create discomfort. It should be noted here that vigorous exercise does not compromise the quantity or composition of breast milk.
Sleep: Seven to nine hours of sleep are recommended for anyone, but it is rare that new mothers get this many hours. Sleep deprivation impairs muscle strength, reduces protein synthesis and increases injury risk in any athlete.
Obesity: is a general risk factor for running injury and should be taken into account (BMI>30 increases injury risk).
Relative Energy Deficiency in Sport (RED-S): RED-S is formerly known as the “female athlete triad”. Energy deficiency occurs when one expends excess energy that is not replenished with adequate nutrition and rest. The post-partum world is full of energy expenditure via breast feeding, sleepless nights and social pressures to return to pre-pregnancy fitness. Adding running into this mix further depletes energy. Without adequate nutrition and rest, the risk of stress fractures, pelvic floor dysfunction and infertility is greatly increased.
Graded return to running
If you pass the above screening, you are ready to return to running! But this doesn’t mean that you lace up and blast out the front door like you used to. What is recommended is a graded return to running. This means slow…literally. The first time you run, it is recommended that you only run for 1-2 minutes at a slow pace. Slow pace means that you can carry on a conversation with a running partner if you needed to. In ramping up your running, you should focus initially on increasing your volume (distance or time spent running), rather than your intensity (how fast you are running). A general guideline is to not increase running volume more than 10% per week. An example of a good program to begin when you are returning to running is a “couch to 5K” program. Such a program gets you up to the 5K distance in about 9 weeks time. An example of a week one starter workout might be 20 minutes total, beginning with a 5 minute brisk walk, and then alternating brisk walking with 90 second bouts of slow running.
Your physical therapist can help
You physical therapist can help you through the above screening process, rehabilitative exercise and a safe, graded return to running. If you need pelvic floor rehab, it is advised that you see a physical therapist who is a pelvic health or women’s health specialist. However, most orthopedic physical therapists can assist you with the first line screening, strength testing and gait analysis. For gait analysis, it is recommended that you see a physical therapist who is experienced in this and understands running biomechanics. Your physical therapist(s) should work in conjunction with your OB/GYN to optimize your rehabilitation program, especially if you have symptoms listed above for pelvic floor and/or abdominal dysfunction.
References:
Goom, Donnelly, and Brockwell. 2019. Returning to running postnatal–guidelines for medical, health and fitness professionals managing this population.
DOI: 10.13140/RG.2.2.35256.90880/2